Successful Right-Sided Azygos Coil Implantation for Failed Defibrillation Thresholds Utilizing a 3D Mapping System

Author: Katherine Romanowicz, CNP
Additional Authors**
See the poster presentation | See the poster
Background: The azygos vein, despite wide anatomical variation, has become an attractive target for coil placement in patients with high or failed defibrillation thresholds as it provides an ideal shock vector. We present a case employing the novel use of 3D mapping for azygos coil placement in a patient with difficult right-sided access.
Case Presentation: A 53 year-old man with heart failure due to ischemic cardiomyopathy (LVEF 10%) with right-sided bi-ventricular ICD implantation and ESRD on dialysis via a left-sided dialysis port was admitted after having episodes of VF at home. His device delivered 3 ineffective shocks, with effective conversion on the 4th shock. Non-invasive program stimulation and DFTs were performed with successful ATP treatment of epicardial VT. DFTs failed, however, in several configurations with maximum output when VF was induced, requiring external defibrillation. Failure was likely due to right-sided device placement and amiodarone therapy. Other risk factors included male gender, wider QRS complex on surface electrocardiogram (200 msec) and CKD. A decision was made to proceed with azygos RV coil implantation.
Discussion: An excessively tortuous right axillary vein and SVC were accessed. A DecaNav catheter and CARTO-Merge were utilized to create a 3D map to locate the azygos vein along with overlap of previously obtained CT angiography. A Decanav and Amplatz catheter were alternatively used for access. The defibrillator coil was placed to the level of the diaphragm and sutured to prepectoral fascia. An adaptor was connected to this lead given it was a DF4 device and a coil had to be added to the DF4 lead. The pocket was expanded to accommodate the adaptor and the leads were coiled behind the device. Ensuing DFTs were successful and there were no procedural complications.
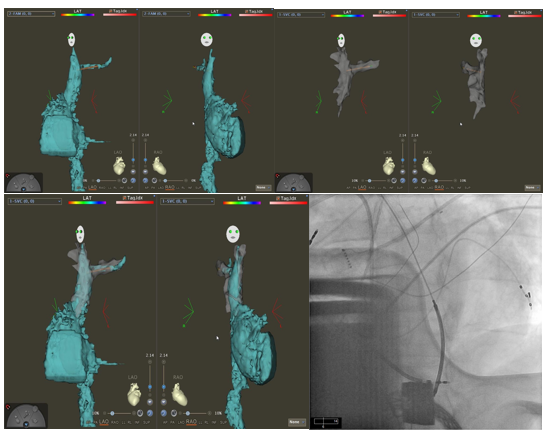
Conclusion: This is a case of successful RV coil insertion in the azygos vein via difficult right-sided access utilizing 3D mapping and overlapping CT angiography. At follow-up, impedance in the azygos coil was measured at 65-68 ohm. To our knowledge, the use of 3D mapping has not been previously used in this application and may provide a valuable tool in future cases.
**Additional Authors:
Katherine Romanowicz, CNP, University of Cincinnati, Cincinnati, Ohio
Muhammad Athar, MD, University of Cincinnati, Cincinnati, Ohio
Alexandru Costea, MD, University of Cincinnati, Cincinnati, Ohio