Acquired Long QT and Torsades De Pointes Induced by Loperamide Toxicity
 Author: Lauren Hassen, MD, MPH, Additional Authors**
Author: Lauren Hassen, MD, MPH, Additional Authors**
See the poster presentation | See the poster
Introduction/Objective: Loperamide is an antidiarrheal agent with peripheral m-opioid receptor activity. When taken in large quantities, loperamide crosses the blood-brain barrier, leading to euphoric and analgesic effects. Between 2010-2015, there was a 91% increase in the nonmedical use of loperamide in the U.S. Abuse has been reported to cause significant cardiotoxicity, including arrhythmias, syncope, and sudden death. We describe a case of acquired long QT interval with recurrent torsades de pointes (TdP) caused by loperamide abuse. In light of the unfortunate epidemic of opioid abuse in Ohio, cardiologists should be informed about loperamide cardiotoxicity.
Case Presentation: A 38-year-old male with a history of past opioid abuse presented to the emergency department with syncope, and was found to be in ventricular tachycardia (VT). He had multiple recurrent episodes of sustained VT, beginning as TdP and organizing into monomorphic VT. He remained hemodynamically stable. His baseline EKG demonstrated sinus bradycardia with frequent premature atrial and ventricular complexes, first degree atrioventricular block, U waves, and prolonged QT and QRS intervals (see figure).
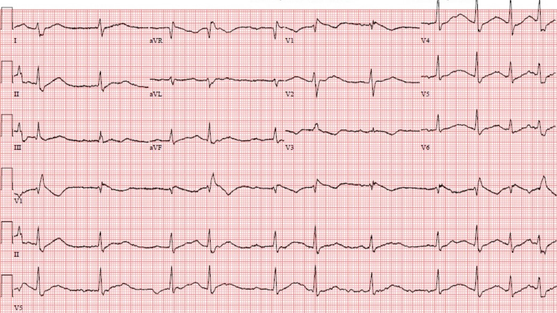
Potassium was 3.1 mg/dL, and magnesium was 1.7 mg/dL. Troponin I was undetectable, and his bedside echocardiogram was largely unremarkable.
Prior to transfer to our institution, he was given an amiodarone bolus as well as atropine. We administered potassium, magnesium and calcium intravenously, as well as a lidocaine bolus and infusion. He underwent multiple synchronized cardioversions. Finally, temporary transvenous pacing (TVP) was initiated with a balloon tipped catheter at 80 beats per minute. VT was successfully terminated, and no further episodes of VT occurred during his hospitalization. Further discussion with the patient and his family revealed that he had been taking approximately 70 pills of loperamide 2mg daily for several months.
Discussion: The arrhythmogenic effects of loperamide are thought to be due to inhibition of both sodium and potassium channels in cardiac myocytes. Loperamide inhibits the sodium channel (NaV1.5) responsible for the fast depolarization current (INa), leading to widening of the QRS interval. Loperamide also antagonizes the human ether-a-go-go (hERG) potassium channel, which regulates the delayed rectifier repolarization current (IKr), prolonging the QT interval. Our case demonstrated both QRS widening and QT prolongation.
There are no evidence-based therapies specifically for loperamide cardiotoxicity. Standard advanced cardiac life support (ACLS) should be implemented for arrhythmias, including cardioversion and prompt correction of electrolyte derangements. Success has been reported with isoproterenol or TVP; an increase in HR can help prevent long-short sequence initiation of TdP until the medication has cleared. Loperamide’s therapeutic half-life is 9-14 hours, but the half-life can be greater than 30 hours in supratherapeutic doses. As loperamide is a lipophilic drug, lipid emulsion has been used in refractory cases to assist with medication clearance. Finally, temporary mechanical support has been utilized in cases with associated cardiogenic shock, including the Impella device and venoarterial extracorporeal membrane oxygenation.
Conclusion: Loperamide overdose can prolong the action potential in cardiac myocytes, causing significant cardiotoxicity. Provider awareness of these effects can facilitate recognition of loperamide toxicity, and thereby help direct appropriate supportive therapies.
**Additional Authors:
Lauren Hassen, MD, MPH, Ohio State University Wexner Medical Center, Columbus, Ohio
Arsheya Patel, MD, Ohio State University Wexner Medical Center, Columbus, Ohio
Chad Ward, MD, Ohio State University Wexner Medical Center, Columbus, Ohio
Steven Kalbfleisch, MD, Ohio State University Wexner Medical Center, Columbus, Ohio