Syncope and Stroke-like Symptoms in a Young Male with Non-Bacterial Thrombotic Endocarditis
Author: Christopher Tanayan MD , Additional authors*
, Additional authors*
Introduction:
- Strokes are rare in young healthy adults.
- Non-Bacterial Thrombotic Endocarditis (NBTE) is also rare.
- We present the case of a young athlete with a stroke secondary to an unexplained non-infectious mitral valve endocarditis.
Case Presentation:
- 20 year-old African American man, college basketball player
- No known medical or surgical history
- CC: Syncopal episode lasting minutes preceded by dizziness
- Transient bilateral vision loss for 15-20 minutes
- Multiple falls at home due to transient loss of sensation in his legs 2 months ago
- ROS: (+) light-headedness (-) fevers, night sweats, chest pain, palpitations, SOB
- No significant family history; Non-smoker, no substance use
- PE: Generally unremarkable. No focal deficits.
- Labs: Normal CMP, CBC, coagulation panel
Case Management:
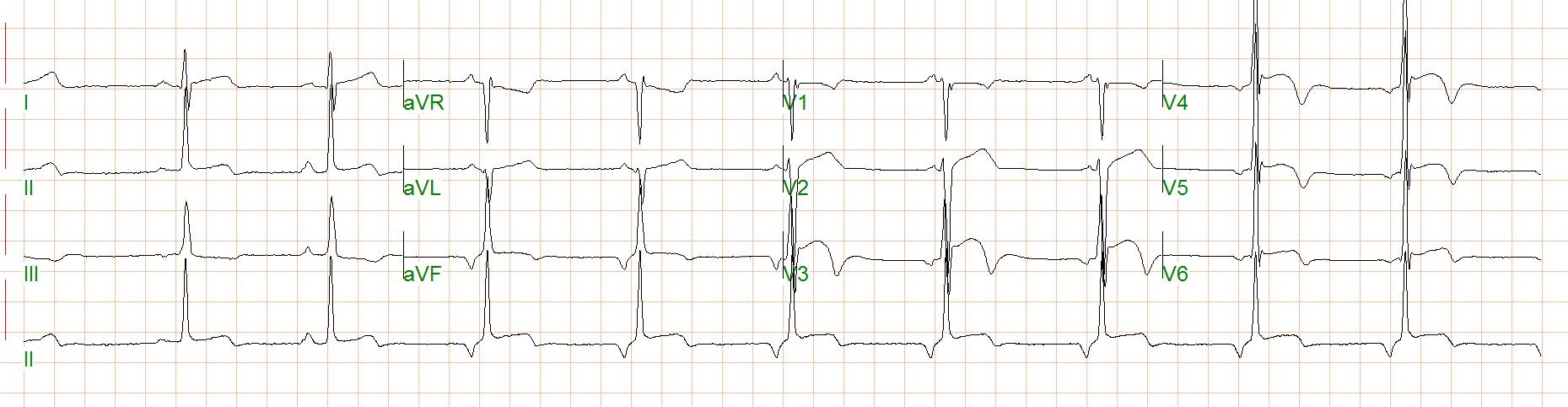
- EKG [Fig 1] was negative for ischemia or arrhythmia.
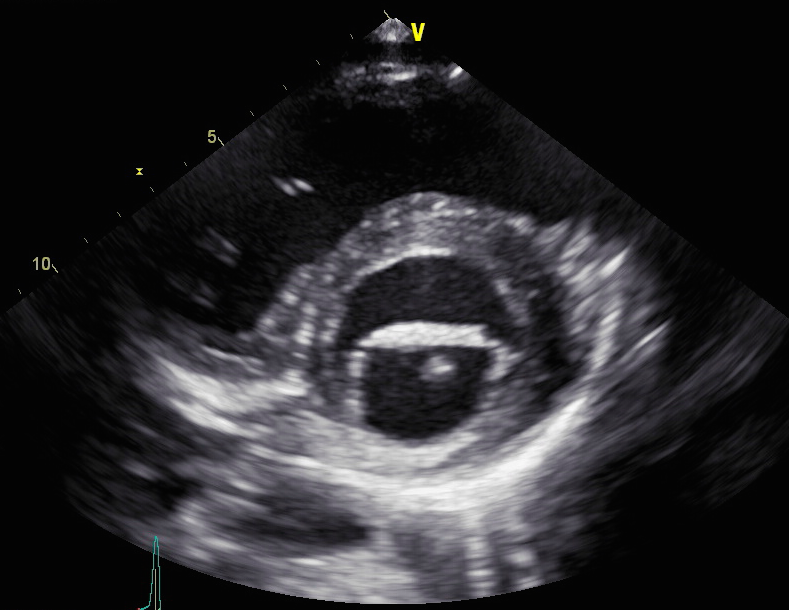
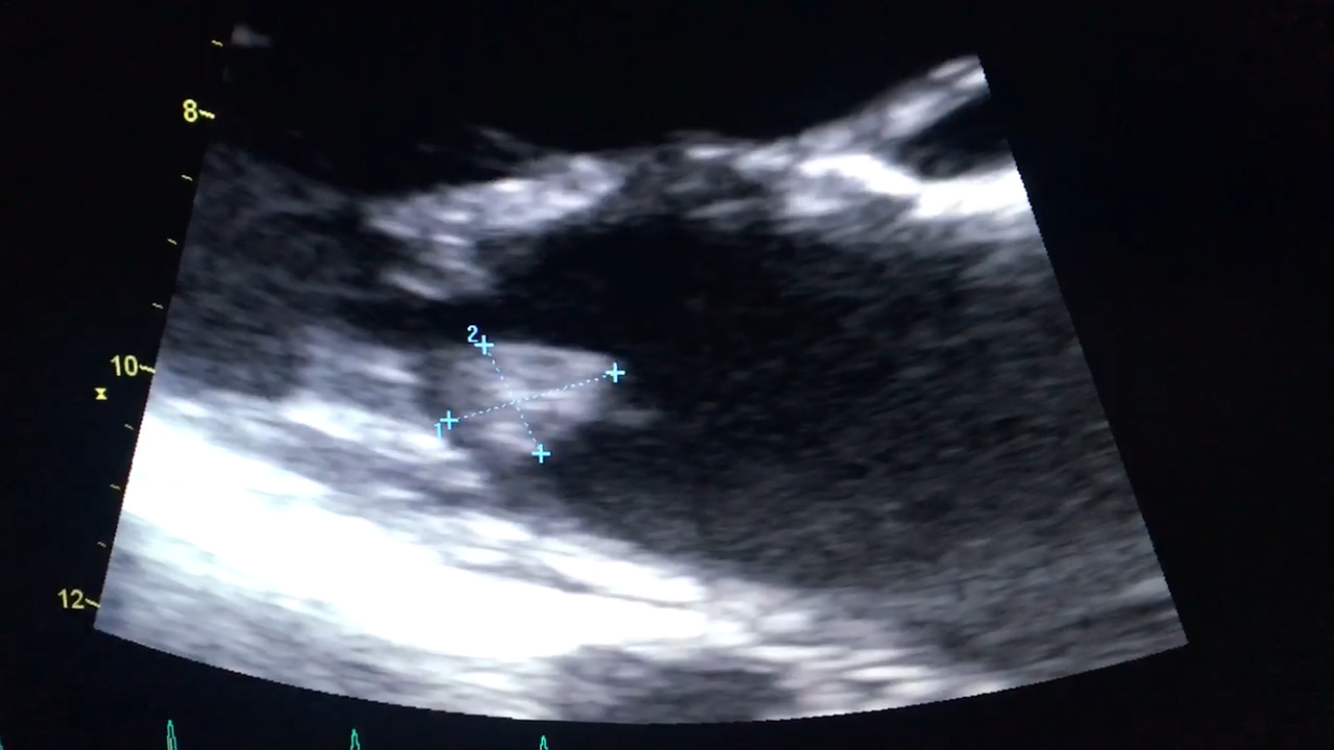
- Trans-esophageal echo [Fig 2,3] showed a mobile mass on the mitral valve. EF was 66% with normal LV function.
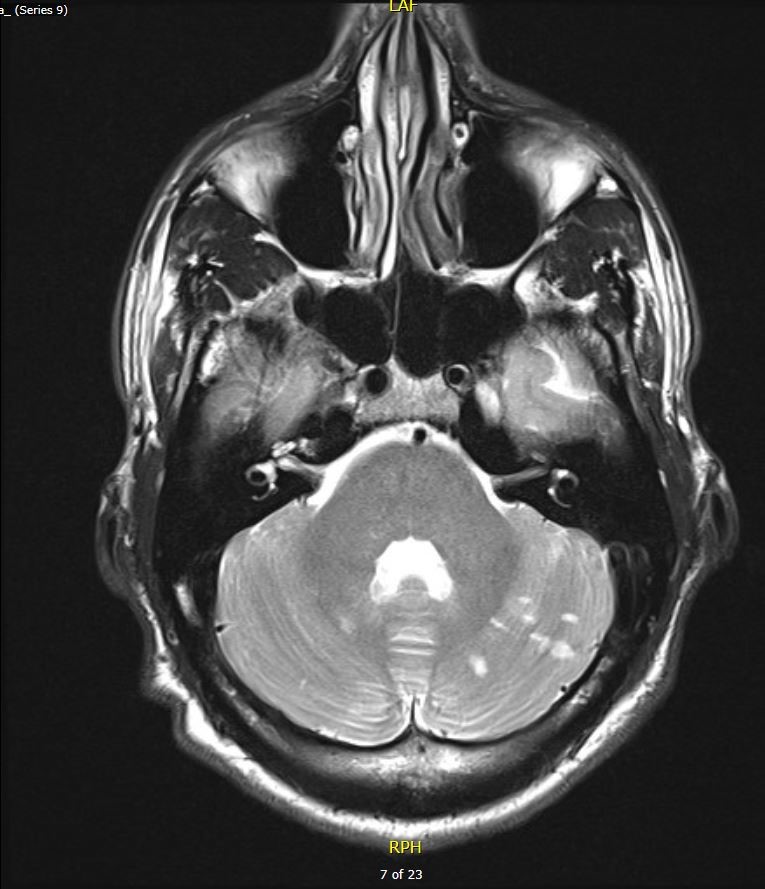
- Brain MRI [Fig 4,5] showed multiple foci of restricted diffusion in bilateral cerebellar hemispheres and the left occipital lobe.
- Emergent debridement and resection of a 0.75 cm mass [Fig 6] from the anterior leaflet and repair of mitral valve with pericardial patch was performed.
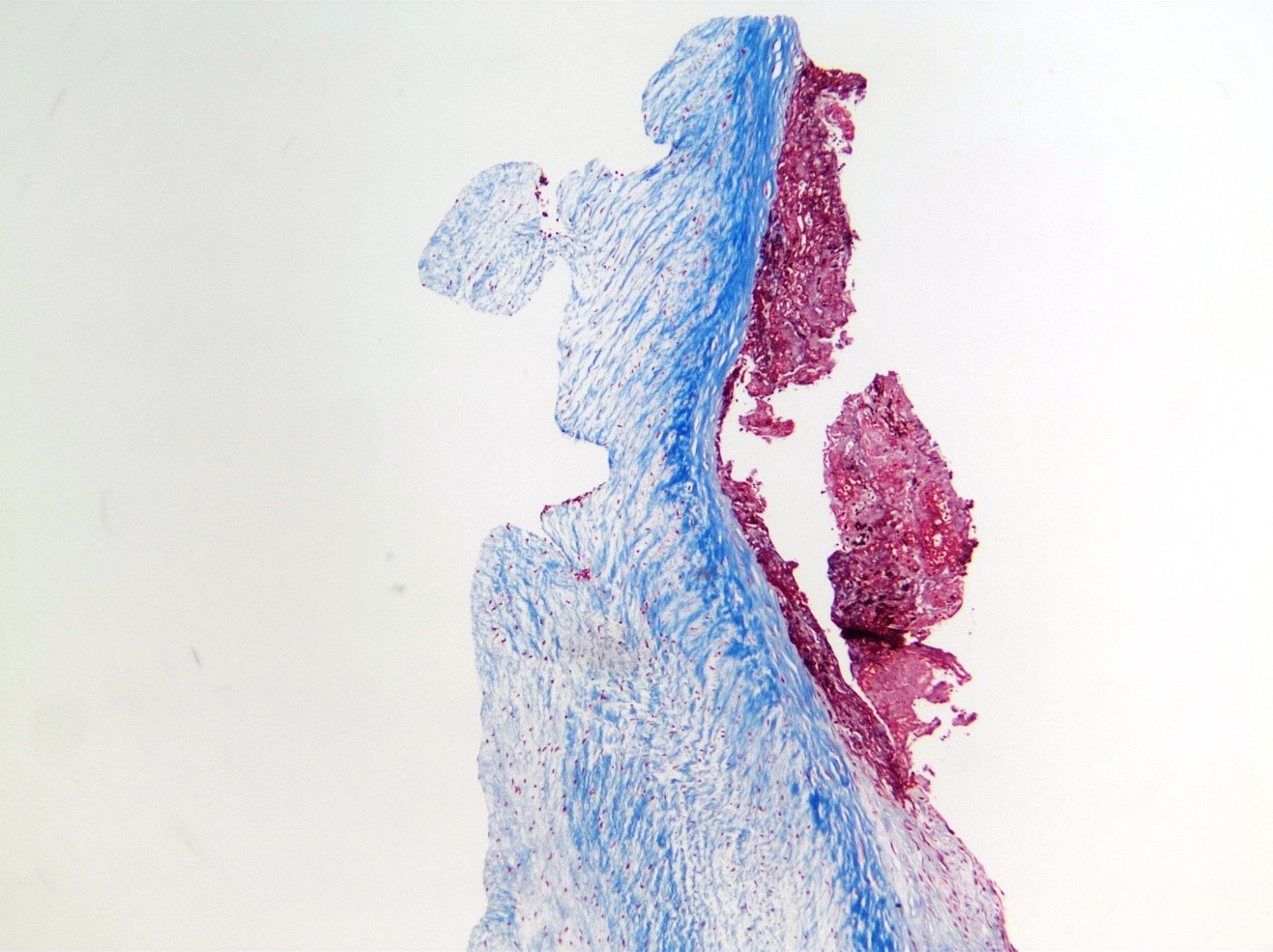
- The mass was sent for pathology evaluation [Fig 7] and cultures. Infectious and rheumatologic work-up was negative.
- On a 3-month follow up transthoracic echo, a new mass was seen on the posterior leaflet of the mitral valve [Fig 8]. The mass resolved after 4 days of anticoagulation.
- He was discharged on indefinite anticoagulation. Extensive outpatient work-up is still inconclusive.
- Lupus, anti-phospholipid antibody syndrome, rheumatoid arthritis, malignancy and other pro-thrombotic conditions have been ruled out.
Discussion:
A cardiac mass must be identified as a tumor or a thrombus for proper management as outlined above [Fig 9].
- Initial evaluation: echocardiography +/- cardiac CT or MRI
- Goal: confirm presence, location, nature of mass
- Tumor was the initial impression of the mass in this case.
- Pathology findings, recurrence and subsequent resolution with anticoagulation proved that this was a thrombus.
Tumor
-
- Myxomas, papillary fibroelastomas and lipomas are the most common benign primary tumors. Secondary tumors are mostly metastatic and rare.
- Symptomatology depend more on the tumor’s location in the heart than on its histopathology.
- Treatment: Regardless of pathology, surgery is recommended if patients are symptomatic (i.e. had embolic events or tumor-related complications).
Thrombus
-
- Culture-negative infectious endocarditis must be ruled out with special stains, PCR, other techniques.
- Non-bacterial thrombotic endocarditis (NBTE, aka marantic, Libman-Sacks, or verrucous endocarditis) is mostly seen in the aortic or mitral valve. It is most commonly associated with advanced malignancy and systemic lupus erythematosus.
- Treatment: anticoagulation to prevent further embolization and addressing the underlying cause.
Conclusion
- This case of NBTE illustrates that this rare entity can occur in the absence of predisposing factors such as rheumatologic disease or pro-thrombotic states.
Though rare, idiopathic cardiac thrombi must be considered in the differential diagnoses of stroke in a young healthy adult.




*Authors
Christopher Tanayan, MD, Summa Health Heart and Vascular Institute – Akron, OH
Akshay Deotare, MD, Summa Health Heart and Vascular Institute – Akron, OH
Yesha Patel, MD, Summa Health Heart and Vascular Institute – Akron, OH
Otto Costantini, MD, Summa Health Heart and Vascular Institute – Akron, OH
Ted Shaub, MD, Summa Health Heart and Vascular Institute – Akron, OH
Program Director: Marc S. Penn, MD, PhD, FACC
Program Coordinator: Sam Lingenfelter