Exaggerated Blood Pressure Response and Outcomes in Asymptomatic Executives Undergoing Exercise Treadmill Testing
 Author: Haris Riaz, MD, Additional authors*
Author: Haris Riaz, MD, Additional authors*
Introduction:
- Exaggerated systolic blood pressure response (ESBPR, >220 mm Hg) during exercise treadmill testing (TMT) is associated with incident hypertension.
- The effect of ESBPR on clinical end points remains unknown.
- We sought to assess whether EBPR adds incremental prognostic value to Reynolds risk score (RRS, a combination of traditional risk factors and c-reactive protein) and exercise capacity in asymptomatic individuals without documented hypertension.
Methods:
- We studied 3401 self-referred, normotensive (excluding documented hypertensives (n=463), asymptomatic subjects patients (mean age 50±7 years, 76% males, 83% Caucasian) presenting for a prospective clinical and TMT evaluation between 1/2005-12/2013. RRS and % age-gender predicted metabolic equivalents (AGP-METs) were calculated.
- Primary endpoint was a combination of death, non-fatal myocardial infarction and stroke (MACE).
Results: Diabetes mellitus, statin use, smoking history and family history of premature coronary disease were present in 2%, 18%, 13% and 9% subjects, respectively. Mean RRS was 3.2±4. ESBPR was observed in 168 (5%) subjects; 97% had normal Duke TMT score and 78% achieved >100% AGP-METs.
- At 7.3±3 years, 67 (2%) had MACE [death in 36 (1%)].
- On multivariable Cox survival analysis, higher RRS (Hazard ratio or HR 1.13 [95% confidence interval or CI 1.09-1.17]), lower% AGP-METs (HR 1.20 [95% CI 1.06-1.35]).
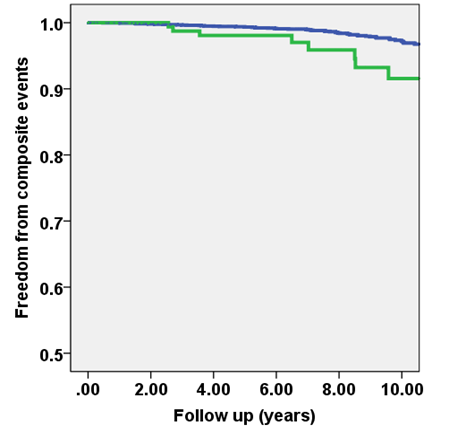
- ESBPR (HR 2.38 [95% CI 1.19-4.38]) were associated with longer-term MACE (all p<0.05).
- Survival curves, separated on ESBPR vs. not, are shown in Figure 1. Findings were similar for longer-term death.
Conclusion:
- In a low-risk asymptomatic cohort, ESBPR is associated with longer term MACE, independent of exercise capacity and standard risk prediction model.
- These findings should be validated in other cohorts.
Translational Outlook: Patients developing ESBPR may represent a subset of patients with higher risk of MACE.
No Disclosures.
*Haris Riaz, Department of Cardiovascular Medicine, Heart and Vascular Institute, Cleveland Clinic Foundation
Alaa Alashi, Department of Cardiovascular Medicine, Heart and Vascular Institute, Cleveland Clinic Foundation
Richard Lang, Department of Cardiovascular Medicine, Heart and Vascular Institute, Cleveland Clinic Foundation
Raul Seballos, Department of Cardiovascular Medicine, Heart and Vascular Institute, Cleveland Clinic Foundation
Steven Feinleib, Department of Cardiovascular Medicine, Heart and Vascular Institute, Cleveland Clinic Foundation
Roxanne Sukol, Department of Cardiovascular Medicine, Heart and Vascular Institute, Cleveland Clinic Foundation
Leslie Cho, Department of Cardiovascular Medicine, Heart and Vascular Institute, Cleveland Clinic Foundation
Paul Cremer, Department of Cardiovascular Medicine, Heart and Vascular Institute, Cleveland Clinic Foundation
Wael Jaber, Department of Cardiovascular Medicine, Heart and Vascular Institute, Cleveland Clinic Foundation
Brian Griffin, Department of Cardiovascular Medicine, Heart and Vascular Institute, Cleveland Clinic Foundation
Milind Desai, Department of Cardiovascular Medicine, Heart and Vascular Institute, Cleveland Clinic Foundation
Program Director: Venugopal Menon, MD, FACC
Program Coordinator: Lois Adamski